Chronic Kidney Disease often leads to the need for dialysis when kidneys can no longer filter waste effectively. Definite Surgical access is crucial for hemodialysis. The Main types of access include:
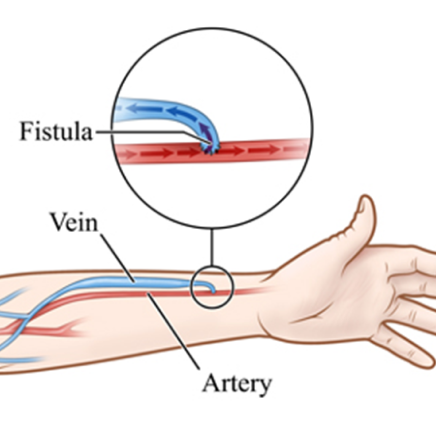
A-V FISTULA
A surgical connection between an artery and a vein, usually in the arm. Considered the best option due to lower infection risk and longer lifespan. Requires time to mature before use, typically 4 to 6 weeks. Venous mapping i.e. identifying the vein most suitable for fistula creation is done by the surgeon at time of surgery.
Catheter Two types
Arteriovenous graft (AV graft)
A synthetic tube implanted to connect an artery and a vein. Used when veins are too small for a fistula. More prone to infection and clotting compared to fistulas.
A conventional dialysis access catheter (tube) is inserted into a large vein, often in the neck. Typically used for short-term access or when immediate dialysis is needed. Higher risk of infection and complications compared to fistulas and grafts.
Another type – Permanent Catheter or Tunneled Dialysis Catheter although inserted into the vein comes out near chest or upper abdomen. It has reduced risk of infection due to the tunnel. It can be used in whom other means of dialysis access have exhausted or as a bridge to another form of access creation.
Care of A-V Fistula / dialysis access
Proper care of the access site is essential to prevent complications such as infections and clots.
Keeping the site clean and dry.
Regularly checking for signs of infection (redness, swelling).
Avoiding drawing of blood or inserting IV cannulas in that arm
Avoid measuring blood pressure in fistula arm
Proper stress ball physio exercise for better maturation of A-V fistula